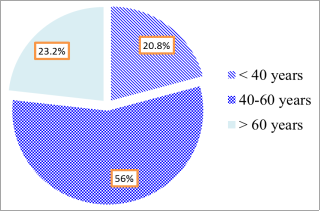
Introduction: male hypogonadism is defined by the European Association of Urology 2022 as being associated with reduced testicular function, reduced androgen production, and/or impaired sperm production. Male hypogonadism has many causes and accompanying diseases such as diabetes, varicocele, etc. Male hypogonadism hadsymptoms of varicocele and had two treatment options: testosterone replacement therapy or surgical treatment of varicocele. Each method has different advantages and disadvantages, so we research to evaluate each treatment method’s results. Objectives: Evaluate the results of male hypogonadism treatment of testosterone replacement therapy or varicocele surgery. Material and methods: conducted a cross-sectional descriptive study in 111 men with symptoms of hypogonadism from January 2022 to the end of 2023. Result: The average age was 65.2 ± 2.4 years. The Androgen Deficiency in Aging Males (ADAM) questionnaire has the highest rate of 90.99% showing symptoms of decreased erection strength. Hypogonadism is associated with body mass index and diabetes. After treatment, the hypogonadism group with grade III varicocele had the lowest response to treatment. After treatment, total testosterone in blood levels in all treatments increased (p<0.001). Conclusion: Testosterone replacement therapy for hypogonadism without varicocele is the gold standard, and microsurgical treatment for hypogonadism with varicocele is the most effective.
| Published in | Journal of Surgery (Volume 12, Issue 5) |
| DOI | 10.11648/j.js.20241205.14 |
| Page(s) | 120-128 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Male Hypogonadism, Testosterone Replacement Therapy (TRT), Varicocele, Varicocelectomy
Accompanying disorders | Frequency (n) | Ratio (%) | |
|---|---|---|---|
Waist circumference (cm) | > 90 | 35 | 31.53 |
76 | 65.47 | ||
Body mass index (Kg/m2) | < 30 | 67 | 60.36 |
≥ 30 | 44 | 39.64 | |
Diabetes | Yes | 36 | 32.43 |
No | 75 | 67.57 | |
Blood lipid disorders | Yes | 48 | 43.24 |
No | 63 | 56.76 | |
Symptoms of androgen deficiency | Frequency (n) | Ratio (%) |
|---|---|---|
Reduced vitality | 24 | 21.62 |
Recently there has been a decline in physical and sports activities | 36 | 32.43 |
Reduce height | 46 | 41.44 |
Bored and/or grumpy | 58 | 52.25 |
Reduced strength and/or endurance | 64 | 57.65 |
Reduced interest in life | 62 | 55.85 |
Feeling sleepy after dinner | 71 | 63.96 |
Reduced sexual desire | 88 | 79.27 |
Reduce labour productivity | 89 | 80.18 |
Reduce erection | 101 | 90.99 |
Total Testosterone | Frequency (n) | Ratio (%) |
|---|---|---|
8-12 nmol/L | 48 | 43.25 |
<8 nmol/L | 63 | 56.75 |
Total | 111 | 100 |
Grade | Total Testosterone concentration (nmol/L) | Frequency (n) | Ratio (%) |
|---|---|---|---|
I | 8.22 | 29 | 26.12 |
II | 6.78 | 23 | 20.72 |
III | 5.56 | 12 | 10.81 |
Without varicocele | 8.32 | 47 | 42.34 |
Characteristic | Testosterone concentration | Total | p | ||
|---|---|---|---|---|---|
8-12 nmol/L | <8 nmol/L | ||||
Body mass index (Kg/m2) | ≥30 | 13 | 31 | 44 | 0.04* |
<30 | 35 | 32 | 67 | ||
Diabetes | Yes | 8 | 28 | 36 | 0.03* |
No | 40 | 35 | 75 | ||
Total | 48 | 63 | 111 | ||
Degree of varicocele | Quantity | Testosterone concentration before treatment (nmol/L) | Testosterone concentration after treatment (nmol/L) | p | ||
|---|---|---|---|---|---|---|
I | 29 | 8.22 | 7.20 | 16.52 | 13.17 | 0.02** |
II | 23 | 6.78 | 12.75 | |||
III | 12 | 5.56 | 5.91 | |||
Without varicocele | 47 | 8.32 | 8.32 | 15.31 | 15.31 | |
Total | 111 | 7.67 | 14.07 | |||
p | 0.04* | 0.01* | ||||
Hypogonadism | Testosterone replacement therapy | Surgery | Total | |
|---|---|---|---|---|
Without varicocele | Varicocele | Varicocele | ||
Sample size | 47 | 31 | 33 | 111 |
Testosterone concentration before treatment (nmol/L) | 8.32 | 8.37 | 6.08 | 7.67 |
Testosterone concentration after treatment (nmol/L) | 15.31 | 12.31 | 13.95 | 14.07 |
p | 0.02* | |||
Side effects | Quantity (n) | Ratio (%) | Side effects | Quantity (n) | Ratio (%) |
|---|---|---|---|---|---|
Diabetes | 3 | 2.70 | Skin reactions | 7 | 6.30 |
Hypertension | 6 | 5.40 | Increased red blood cells | 18 | 16.21 |
Headache | 8 | 7.20 | Total | 42 | 37.83 |
| [1] |
Salonia A, Minhas S. EAU Guidelines on Sexual and Reproductive Health. Edn. Presented at the EAU Annual Congress Amsterdam. EAU Guidelines Office Arnhem. 2022. The Netherlands.
https://uroweb.org/guidelines/sexual-and-reproductive-health |
| [2] | Sebo ZL, Rodeheffer MS. Testosterone metabolites differentially regulate abiogenesis and fat distribution. Mol Metab. 2021 Feb; 44: 101141. |
| [3] | Li F, Yue H, Yamaguchi K, Okada K, Matsushita K, Ando M, Chiba K, Fujisawa M. Effect of surgical repair on testosterone production in infertile men with varicocele: a meta-analysis. Int J Urol. 2012 Feb; 19(2): 149-54. |
| [4] | Çayan S, Akbay E, Saylam B, Kadıoğlu A. Effect of Varicocele and Its Treatment on Testosterone in Hypogonadal Men with Varicocele: Review of the Literature. Balkan Med J. 2020 Apr 10; 37(3): 121-124. |
| [5] | Dubin L, Amelar RD. Varicocele size and results of varicocelectomy in selected subfertile men with varicocele. Fertil Steril. 1970 Aug; 21(8): 606-9. |
| [6] | Bertolotto M, Cantisani V, Drudi FM, Lotti F. Varicocoele. Classification and pitfalls. Andrology. 2021 Sep; 9(5): 1322-1330. |
| [7] | Chen W, Liu ZY, Wang LH, Zeng QS, Wang HQ, Sun YH. Are the Aging Male's Symptoms (AMS) scale and the Androgen Deficiency in the Aging Male (ADAM) questionnaire suitable for the screening of late-onset hypogonadism in aging Chinese men? Aging Male. 2013 Sep; 16(3): 92-6. |
| [8] | Panach-Navarrete J, Morales-Giraldo A, Ferrandis-Cortés C, García-Morata F, Pastor-Lence JC, Martínez-Jabaloyas JM. Is there a relationship between varicocele and testosterone levels? Aging Male. 2020 Dec; 23(5): 592-598. |
| [9] | Huhtaniemi I, Forti G. Male late-onset hypogonadism: pathogenesis, diagnosis and treatment. Nat Rev Urol. 2011 Apr 19; 8(6): 335-44. |
| [10] | Clavijo RI, Carrasquillo R, Ramasamy R. Varicoceles: prevalence and pathogenesis in adult men. Fertil Steril. 2017 Sep; 108(3): 364-369. |
| [11] | Dachille G, Ludovico GM, Pagliarulo G, Vestita G. Sexual dysfunctions in multiple sclerosis. Minerva Urol Nefrol. 2008 Jun; 60(2): 77-9. |
| [12] | Ji B, Jin XB. Varicocele is associated with hypogonadism and impaired erectile function: a prospective comparative study. Andrologia. 2017 Aug; 49(6). |
| [13] | Domes T, Najafabadi BT, Roberts M, Campbell J, Flannigan R, Bach P, Patel P, Langille G, Krakowsky Y, Violette PD. Canadian Urological Association guideline: Erectile dysfunction. Can Urol Assoc J. 2021 Oct; 15(10): 310-322. |
| [14] | Corona G, Goulis DG, Huhtaniemi I, Zitzmann M, Toppari J, Forti G, Vanderschueren D, Wu FC. European Academy of Andrology (EAA) guidelines on investigation, treatment and monitoring of functional hypogonadism in males: Endorsing organization: European Society of Endocrinology. Andrology. 2020 Sep; 8(5): 970-987. |
| [15] | Hackett G, Kirby M, Coxon J, Muneer A; British Society for Sexual Medicine. Letter - ED guideline needs more focus on patient-centered management Re: CUA guideline: Erectile dysfunction, CUAJ, Oct 2021. Can Urol Assoc J. 2021 Dec; 15(12): 425. |
| [16] | Tanrikut C, Goldstein M, Rosoff JS, Lee RK, Nelson CJ, Mulhall JP. Varicocele as a risk factor for androgen deficiency and effect of repair. BJU Int. 2011 Nov; 108(9): 1480-4. |
| [17] | Al-Ali BM, Marszalek M, Shamloul R, Pummer K, Trummer H. Clinical parameters and semen analysis in 716 Austrian patients with varicocele. Urology. 2010 May; 75(5): 1069-73. |
| [18] | Thanaboonyawat I, Chera-aree P, Petyim S, Choavaratana R, Laokirkkiat P. The effect of three-month topical testosterone gel application on semen quality in men with oligozoospermia and low serum testosterone levels. Clin. Exp. Obstet. Gynecol. 2020, 47(6), 875–881. |
| [19] | Ramasamy R, Scovell JM, Kovac JR, Lipshultz LI. Testosterone supplementation versus clomiphene citrate for hypogonadism: an age matched comparison of satisfaction and efficacy. J Urol. 2014 Sep; 192(3): 875-9. |
| [20] | Hsiao W, Rosoff JS, Pale JR, Powell JL, Goldstein M. Varicocelectomy is associated with increases in serum testosterone independent of clinical grade. Urology. 2013 Jun; 81(6): 1213-7. |
| [21] | Zohdy W, Ghazi S, Arafa M. Impact of varicocelectomy on gonadal and erectile functions in men with hypogonadism and infertility. J Sex Med. 2011 Mar; 8(3): 885-93. |
| [22] | Whelan P, Levine L. Effects of varicocelectomy on serum testosterone. Transl Androl Urol. 2016 Dec; 5(6): 866-876. |
| [23] | Wittert GA, Harrison RW, Buckley MJ, Wlodarczyk J. An open-label, phase 2, single centre, randomized, crossover design bioequivalence study of AndroForte 5 testosterone cream and Testogel 1% testosterone gel in hypogonadal men: study LP101. Andrology. 2016 Jan; 4(1): 41-5. |
| [24] | Vinarov AZ, Rozhivanov RV. [Effect of transdermal testosterone on the quality of life of men with androgen deficiency and chronic prostatitis in routine clinical practicea]. Urologiia. 2018 Mar; (1): 71-76. Russian. |
| [25] | Meikle AW, Arver S, Dobs AS, Sanders SW, Rajaram L, Mazer NA. Pharmacokinetics and metabolism of a permeation-enhanced testosterone transdermal system in hypogonadal men: influence of application site- -a clinical research center study. J Clin Endocrinol Metab. 1996 May; 81(5): 1832-40. |
| [26] | Corona G, Rastrelli G, Forti G, Maggi M. Update in testosterone therapy for men. J Sex Med. 2011 Mar; 8(3): 639-54; quiz 655. |
APA Style
Hieu, N. T., Kien, N. T., Cuong, D. V., Binh, L. T., Cuong, T. Q., et al. (2024). Evaluation of Treatment Results for Male Hypogonadism in Patients with Varicocele and Without Varicocele in Can Tho City. Journal of Surgery, 12(5), 120-128. https://doi.org/10.11648/j.js.20241205.14
ACS Style
Hieu, N. T.; Kien, N. T.; Cuong, D. V.; Binh, L. T.; Cuong, T. Q., et al. Evaluation of Treatment Results for Male Hypogonadism in Patients with Varicocele and Without Varicocele in Can Tho City. J. Surg. 2024, 12(5), 120-128. doi: 10.11648/j.js.20241205.14
AMA Style
Hieu NT, Kien NT, Cuong DV, Binh LT, Cuong TQ, et al. Evaluation of Treatment Results for Male Hypogonadism in Patients with Varicocele and Without Varicocele in Can Tho City. J Surg. 2024;12(5):120-128. doi: 10.11648/j.js.20241205.14
@article{10.11648/j.js.20241205.14,
author = {Nguyen Trung Hieu and Nguyen Trung Kien and Dam Van Cuong and Le Thanh Binh and Tran Quoc Cuong and Hoang Minh Tu and Luong Tieu Yen},
title = {Evaluation of Treatment Results for Male Hypogonadism in Patients with Varicocele and Without Varicocele in Can Tho City
},
journal = {Journal of Surgery},
volume = {12},
number = {5},
pages = {120-128},
doi = {10.11648/j.js.20241205.14},
url = {https://doi.org/10.11648/j.js.20241205.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20241205.14},
abstract = {Introduction: male hypogonadism is defined by the European Association of Urology 2022 as being associated with reduced testicular function, reduced androgen production, and/or impaired sperm production. Male hypogonadism has many causes and accompanying diseases such as diabetes, varicocele, etc. Male hypogonadism hadsymptoms of varicocele and had two treatment options: testosterone replacement therapy or surgical treatment of varicocele. Each method has different advantages and disadvantages, so we research to evaluate each treatment method’s results. Objectives: Evaluate the results of male hypogonadism treatment of testosterone replacement therapy or varicocele surgery. Material and methods: conducted a cross-sectional descriptive study in 111 men with symptoms of hypogonadism from January 2022 to the end of 2023. Result: The average age was 65.2 ± 2.4 years. The Androgen Deficiency in Aging Males (ADAM) questionnaire has the highest rate of 90.99% showing symptoms of decreased erection strength. Hypogonadism is associated with body mass index and diabetes. After treatment, the hypogonadism group with grade III varicocele had the lowest response to treatment. After treatment, total testosterone in blood levels in all treatments increased (pConclusion: Testosterone replacement therapy for hypogonadism without varicocele is the gold standard, and microsurgical treatment for hypogonadism with varicocele is the most effective.
},
year = {2024}
}
TY - JOUR T1 - Evaluation of Treatment Results for Male Hypogonadism in Patients with Varicocele and Without Varicocele in Can Tho City AU - Nguyen Trung Hieu AU - Nguyen Trung Kien AU - Dam Van Cuong AU - Le Thanh Binh AU - Tran Quoc Cuong AU - Hoang Minh Tu AU - Luong Tieu Yen Y1 - 2024/10/18 PY - 2024 N1 - https://doi.org/10.11648/j.js.20241205.14 DO - 10.11648/j.js.20241205.14 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 120 EP - 128 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20241205.14 AB - Introduction: male hypogonadism is defined by the European Association of Urology 2022 as being associated with reduced testicular function, reduced androgen production, and/or impaired sperm production. Male hypogonadism has many causes and accompanying diseases such as diabetes, varicocele, etc. Male hypogonadism hadsymptoms of varicocele and had two treatment options: testosterone replacement therapy or surgical treatment of varicocele. Each method has different advantages and disadvantages, so we research to evaluate each treatment method’s results. Objectives: Evaluate the results of male hypogonadism treatment of testosterone replacement therapy or varicocele surgery. Material and methods: conducted a cross-sectional descriptive study in 111 men with symptoms of hypogonadism from January 2022 to the end of 2023. Result: The average age was 65.2 ± 2.4 years. The Androgen Deficiency in Aging Males (ADAM) questionnaire has the highest rate of 90.99% showing symptoms of decreased erection strength. Hypogonadism is associated with body mass index and diabetes. After treatment, the hypogonadism group with grade III varicocele had the lowest response to treatment. After treatment, total testosterone in blood levels in all treatments increased (pConclusion: Testosterone replacement therapy for hypogonadism without varicocele is the gold standard, and microsurgical treatment for hypogonadism with varicocele is the most effective. VL - 12 IS - 5 ER -
Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho City, Viet Nam